An 18-Month Randomized Clinical Trial with I-ReHealth Fluoride VarnishIssuing time:2023-02-01 15:33 This was a single-blind randomized controlled clinical trial. A convenience sample of participants was recruited while having routine treatment in the local Faculty’s Paediatric Dental Clinic during the period Sep/2016 to Jan/2017. The sample size was calculated based on the relative risk of PEB development in a total of 185 MIH-affected permanent incisors and first molars of 45 children that received FV applications weekly over 1 month. Results reported being 2% for yellow and 17% for brown opacities at 1-year follow-up. Given two experimental proportions design, a minimal of 62 teeth would be required for FV intervention to achieve a power of 0.85 at a 5% significance level. Considering a dropout rate of 20% and three experimental protocols, it was determined that at least 202 teeth would be required for all interventions.
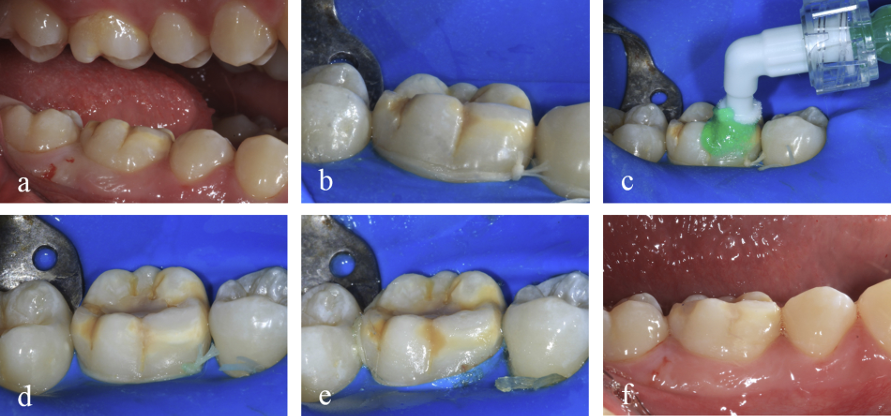
Fig. 1. Resin infiltration performed in MIH-affected molar. a) initial clinical aspect; b) rubber dam isolation after local anaesthesia and prophylaxis; c) enamel conditioning with Icon Etch for 2 min; d) rinsing, drying, and application of Icon Dry for 30 s; e) two applications of Icon Infiltrant for 2 min and light-curing for 40 s; f) Rubber dam removal and final aspect of the opacity. A total of 223 children aged from 6 to 12-years were examined to determine whether the participants met the inclusion and exclusion criteria. Examinations were performed by a calibrated researcher (A) in the dental clinical environment using a triple syringe and a reflector light. Participants returned at 1, 3, 6, 12, and 18 months after interventions. At these periods, VPI and DMFT were reassessed by the researcher (A), who was fully blinded regarding the assigned interventions. The teeth were photographed to compare enamel structural integrity throughout the subsequent evaluations (Fig. 2). The cut-off for the presence of carious lesions (CL) was determined using an ICDAS score ≥3, due to the difficulty of differentiating white spots lesions masked by MIH lesions. The same oral hygiene instructions given on the day of treatment were reinforced at all reassessments.
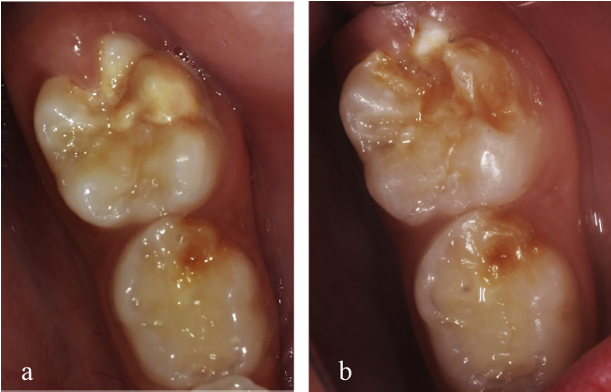
Fig. 2. Clinical aspect of a MIH-affected tooth (yellow opacity) treated with fluoride varnish therapy (FV) at a) baseline and b) after an 18-month follow-up period (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article). At baseline, 54 children were included in the study, totalling 249 teeth, randomly allocated at FV: 86 teeth; FV+etch: 81 teeth; RI: 82 teeth (Fig. 3). Throughout the study, three children withdrew their participation. Thus, at the end of 18 months, 51 participants were evaluated: 50.9% were female, the mean age was 8.1 years (median = 8.2). The teeth distribution was FV: 45 molars and 33 incisors; FV+etch: 43 molars and 32 incisors; RI: 47 molars and 35 incisors, with a mean value of 4±2 (±SD) affected teeth per participant.
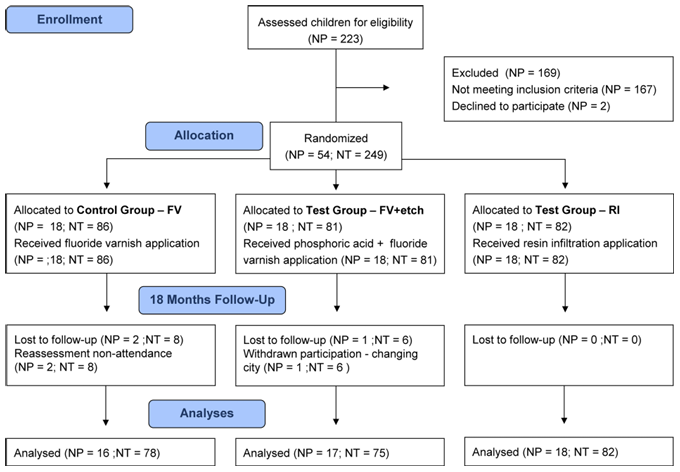
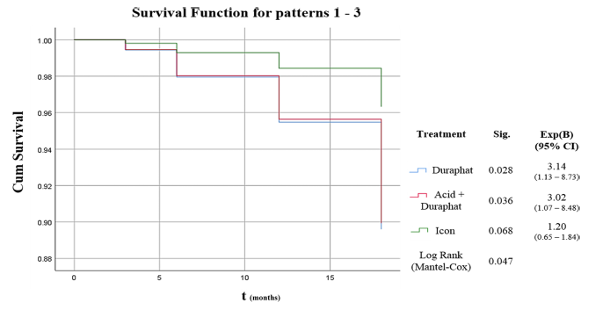
Fig. 3. CONSORT flow diagram of trial enrolment. NP: Number of patients, NT: Number of teeth. After the 18-months assessments, the frequency of failure was 17.9% for FV, 17.3% for FV+etch, and 6.10% for RI, the latter being significantly lower (Fisher’s Exact test; p<0.05). Failures prevailed in molars. Carious lesions development (CL) occurred only associated with PEB and for molars treated with FV (2 teeth; 4.4%) or FV+etch (1 tooth, 2.3%). The survival of FV and FV+etch was significantly lower compared to RI at 6 months (Mantel-Cox; p=0.04), and presented an increased risk of failure of 3.1 (OR) and 3.0 (OR), respectively (p<0.05; Fig. 4).
Fig. 4. Kaplan-Meier survival curves and Cox regression of failure development of MIH-affected teeth according to the intervention group throughout 18-months follow-up. Significance level at five percent. DMFT, opacity colour, tooth surface, and age were significantly associated with failure (Fisher’s Exact Test; p<0.05). Participants aged 6–9 years presenting DMFT >3, brown opacities, and cusp involvement together presented the lowest survival rates in all follow-up sessions, especially at 18 months (FV: 10.7%; FV+etch: 10.4%; and RI: 20.2%). Among the strategies evaluated, resin infiltration positively influenced the structural integrity of MIH-affected teeth by decreasing the risk of enamel breakdown after18 months follow-up. |