Efficacy and Cost Analysis of Two Fluoride Varnishes in Community-Based Interventions for Early Childhood CariesIssuing time:2026-01-13 11:50 Yang Chaoqing, Yu Jinmei, Zhang Yishan, Liu Fanghong, Pang Qiuling, Xie Yulu, Ran Lingshan, Qiu Rongmin 1. College & Hospital of Stomatology, Guangxi Medical University, Guangxi Key Laboratory of the Rehabilitation and Reconstruction for Oral and Maxillofacial Research, Guangxi Clinical Research Center for Craniofacial Deformity, Guangxi Health Commission Key Laboratory of Prevention and Treatment for Oral Infectious Diseases, Nanning 530021, China; 2. Dept. of Stomatology, The People's Hospital of Hechi, Hechi 547000, China Supported by: Key Research and Development Project of Guangxi Science and Technology Department (AB22035015); Guangxi Medical and Health Appropriate Technology Development and Promotion and Application Project (S2020041, S2024121); Key Research and Development Program of Science and Technology Plan Project of Qingxiu District, Nanning (2020039) Abstract Abstrac Objective: A community intervention model was used to investigate the preventive effects and cost-effectiveness of I-ReHealth? and Duraphat? in early childhood caries. Methods: Children from Yizhou District, Hechi City, were enrolled and randomly assigned in to two groups: the I-ReHealth? (China) group and the Duraphat? (Colgate, USA) group. Each group received topical fluoride varnish applications and dental health education every 6 months. After 1.5 years, the incidence of caries and associated costs were compared between the two groups before and after the intervention. Cost minimization analysis was employed to evaluate economic efficiency, and sensitivity analysis was performed to assess the influence of variations in key parameters on result stability and to quantify the probabilistic differences in cost benefits between the two fluoride varnishes under equivalent caries-preventive effects. Results: Prior to the intervention, we found no statistically significant differences in caries prevalence or mean dmft scores between the two groups (P>0.05). After 1.5 years of treatment, both groups still showed no statistically significant differences in caries prevalence (P>0.05), mean dmft scores (P>0.05), caries incidence rate (P>0.05), or increment in mean dmft (P>0.05). The one-sided 97.5% confidence interval for the difference in mean dmft increment was below the non-inferiority threshold, confirming non-inferiority (P<0.025). Cost minimization analysis revealed lower total costs in the I-ReHealth? group (¥25 411.44) than in the Duraphat? group (¥26 692.98). One-way sensitivity analysis identified material price as the most influential parameter affecting total costs. Monte Carlo simulation with 1 000 iterations demonstrated a 73.1% probability that the I-ReHealth? group will yield cost savings compared with the Duraphat? group. Conclusion: I-ReHealth? is non-inferior to Duraphat? in caries-preventive efficacy but superior in cost-effectiveness in reducing patient expenses. Keywords Early childhood caries; Fluoride varnish; Community-based intervention; Cost minimization analysis CLC Number: R780.1; Document Code: A; doi: 10.7518/hxkq.2026.2025174
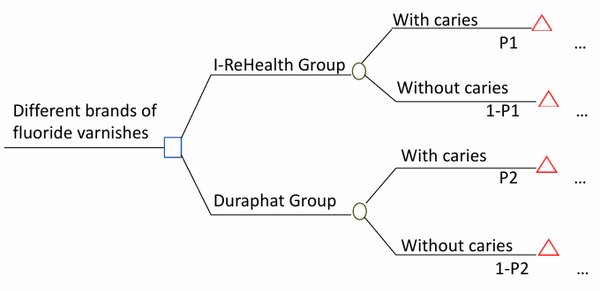
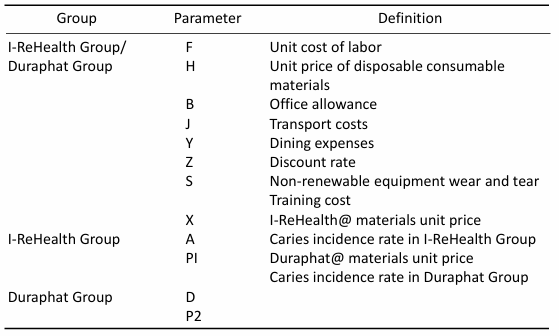
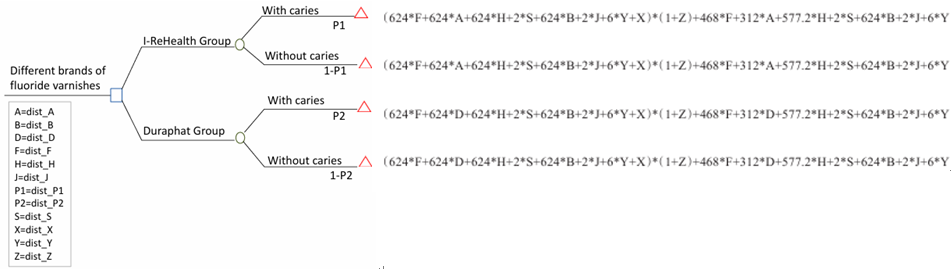
Dental caries, as a chronic non-communicable disease, has become a major global public health problem, affecting human oral health. The prevalence of dental caries among young children in Guangxi is particularly severe. The Fourth National Epidemiological Survey of Oral Health shows that the prevalence of dental caries in deciduous teeth among children aged 3-5 years in Guangxi is as high as 72.3%, which is nearly 10 percentage points higher than the national average for the same age group (62.5%). Dental caries not only causes health problems such as pain and chewing dysfunction, but its treatment costs also place a heavy economic burden on families and society. Among many preventive measures, topical application of fluoride varnish is recommended by the World Health Organization (WHO) as the preferred intervention for community prevention and control of dental caries in children because of its high concentration of fluoride (22,600 ppm) acting directly on the tooth surface, its simple operation, and its safety and effectiveness. With the deepening of China's new medical reform policy, medical institutions urgently need to consider both cost-effectiveness and prevention and control efficiency in the use of consumables. This policy orientation makes the search for fluoride varnishwith significant anti-caries effecacy and excellent cost performance an urgent need in the current public health field. In recent years, breakthroughs in R&D of domestically produced fluorinated coatings (such as I-ReHealth@) have provided new options for community caries prevention programs. Their price advantage makes them a potential alternative to traditional imported products (such as Duraphate@). However, the lack of systematic effectiveness comparisons and economic evaluations may lead to improper allocation of public health resources, thereby affecting the effectiveness of dental prevention among the population. Currently, there is a significant gap in comparative studies of different fluorinated coatings both domestically and internationally: on the one hand, existing studies mostly focus on comparing the clinical efficacy verification and cost-benefit assessment of single-brand fluorine-coatings with and without intervention; on the other hand, the few relevant studies in China have not yet established a complete cost-effectiveness analysis framework. This study innovatively adopts a community intervention trial design to comparatively analyze the caries preventiive effects and costs of I-ReHealth@'s fluoride varnish, which is widely used in Guangxi, and the classic product Duraphat@. It provides a scientific basis for selecting the optimal cavity prevention intervention plans for regional children's dental caries prevention, optimizing the allocation of public health resources, and formulating material procurement strategies that are in line with the principle of cost-effectiveness. 1. Materials and Methods 1.1 Research subject Eight kindergartens with similar geographical locations, dietary habits and educational conditions in Yizhou District, Hechi City, Guangxi Province were selected. Children aged 3 years old and their main caregivers from these kindergartens were chosen as the research subjects. Inclusion criteria: 1) The parents/ guardians of the children have given informed consent and are willing to participate in this study; 2) During the study, the children were willing to cooperate with the examinations. Exclusion criteria: 1) Children with a history of asthma or allergic to fluoride or rosin; 2) Children with a strong vomiting reflex; 3) Children with ulcerative gingivitis or herpes stomatitis. College & Hospital of Stomatology, Guangxi Medical University (approval number: 2023047) and the Clinical Research Ethics Committee of The People's Hospital of Hechi (approval number: 2024-111-01), and was registered in the National Clinical Trial Center (registration number: ChiCTR2500099748). The study period was from March 2023 to September 2024. 1.2 Sample size and sampling method Sample size formula: In the formula, n: two groups of overall samples: Based on the previous research of the research group (the additional caries caused by the regular intervention of Doraphat@ was 2.86 ± 2.83) [10], combined with the non-inferiority threshold in the statistical textbook, it can be appropriately set as 1/5 to 1/2 of a standard deviation, and consulting with oral experts, the Δ value is set as 3/10 of the standard deviation of the additional caries caused by the regular intervention of dDoraphat@, therefore Δ = 0.849, σ = 2.83, δ = 0, k = 0.5, α = 0.025 (one-sided test level), β = 0.1. Substituting these values into the formula for calculation, considering a 10% sample loss rate, it is calculated that each group requires at least 260 people as the sample size. A two-stage random sampling method was adopted, and the hidden allocation method was used to randomly divide 8 kindergartens into the I-ReHealth group (experimental group) and the Duraphat group (control group). A single-blind design was implemented for 3-year-old children whose parents gave informed consent and met the inclusion criteria. A total of 664 children were included in the research sample, with 327 in the I-ReHealth group and 337 in the Duraphat group. 1.3 Intervention Through questionnaire surveys, information on the demographic and socio-economic indicators, dietary habits, and oral health behaviors of children was obtained from their primary caregivers. Three inspectors, who had received professional training, had Kappa values greater than 0.88 for the examinations of dental caries, enamel hypoplasia, and visible plaque. The experimental group used the I-ReHealth? fluoride varnish (Approval Number: 20202170057, produced by Chengdu I-ReHealth Medical Devices Co., Ltd., 10 grams per pack), whose main components are 5% sodium fluoride, ethanol, pine resin, gum arabic, white beeswax, frankincense extract, sodium saccharin, raspberry flavoring. The control group used the Duraphat? fluoride varnish (Approval Number: 20152173181, produced by Colgate (China) P&G Co., Ltd., 10 grams per pack), whose main components are 5% sodium fluoride, ethanol, pine resin, white wax, resin, frankincense, saccharin, flavoring, etc. I-ReHealth Group: Oral health education, re-examination and professional fluoride application were conducted every 6 months. A total of 3 fluoride applications were carried out, at the baseline, 6 months later and 1 year later. Before the operation, children were instructed to rinse their mouths thoroughly with water, dry the tooth surfaces with a cotton swab, and use I-ReHealth@ as the fluoride coating. According to the instructions, the usage amount for each person should not exceed 0.25 g. Use a small brush to evenly apply the fluoride varnish on each dry tooth surface. After the application, instruct the children not to rinse their mouths, drink or eat within 30 minutes, allowing it to fully solidify. Avoid eating hard foods within 4 hours. Do not brush their teeth on the night of the fluoride application. Duraphat Group: Oral health education, re-examination and professional fluoride application were conducted every 6 months. A total of 3 fluoride applications were carried out, at the baseline, 6 months later and 1 year later. Use Duraphat@ as the fluoride coating, the operation method is the same as that of the I-ReHealth group. 1.4 Data entry and statistical analysis The data were double-checked and double-entered using EpiData 3.0 software to ensure the accuracy of information entry. Data were imported, organized, and statistically analyzed using SPSS 26.0 software. The comparison of the rates of two independent samples was conducted using Pearson's chi-square test or continuity correction; since the index of dental caries loss and restoration for primary teeth did not follow a normal distribution, the comparison of the means of the two samples was performed using non-parametric tests (Mann-Whitney U test), but the mean and standard deviation were used to describe the mean caries per tooth in accordance with the WHO's expression method. The significance level was two-sided α = 0.05; if P < 0.05, it was considered that the difference was statistically significant. The SAS 9.4 software was used to conduct a non-inferiority test for the most sensitive indicator of dental caries, with the test level being one-sided α = 0.025; if P < 0.025, it was considered that the non-inferiority conclusion was established. The specific analysis methods for cost-effectiveness evaluation are as follows. 1) Cost determination. The pharmacoeconomic evaluation of public decisions should be conducted from a societal perspective. Therefore, this study estimates the costs from a societal perspective. Cost estimation includes all direct medical costs, direct non-medical costs, and indirect costs, such as the human cost, material cost, operational cost, and indirect cost generated during the project implementation process. 2) Health economics evaluation. The main evaluation methods in health economics are four: cost-effectiveness analysis (CEA), cost-benefit analysis (CBA), cost-utility analysis (CUA), and cost-minimization analysis (CMA). If the evidence from this study shows that the two fluoridevarnishes have the same efficacy and safety or no clinically significant differences, the cost-minimization analysis method can be selected for economic evaluation. At this time, it can be considered that the cost of choosing which fluoride varnish for prevention is lower, and it is a more economically advantageous choice. 3) Model analysis. A decision tree model was constructed using the TreeAge Pro 2022 software. The model structure is shown in Figure 1, and the model parameters are presented in Table 1.
Fig 1 The decision tree model 4) Cost estimation. A total of 4 follow-up visits were conducted in kindergartens within 1.5 years. All the costs for the year 2023 were discounted at a rate of 5% for present value calculation. The discount calculation formula is: Pv = Pc × (1 + r)^n, where Pv is the present value of the cost, Pc the past value of the cost or effect, r the annual discount rate, and n the time period. Taking 2024 as the base year, the present value of the 2023 cost is: Pv = Pc × (1 + r)^1, and the costs generated in 2024 do not need to be discounted. 5) Sensitivity analysis. Within all parameter variations, single-factor sensitivity analysis and probabilistic sensitivity analysis are employed to analyze the uncertainties in the economic evaluation, in order to determine the impact of the data on the research conclusions. Among various indicators, the cost parameters fluctuate within ±20%, the effect parameters are taken as the upper and lower limits of the 95% confidence interval (CI), and the discount rate ranges from 0% to 8%. Tab 1 Model parameters composition
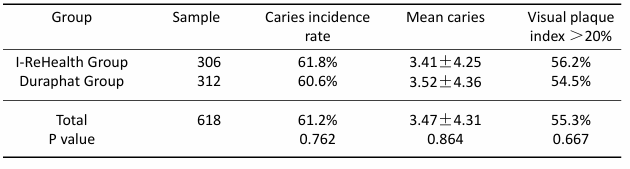
2. Results 2.1 Baseline condition At the baseline, a total of 664 children were included in the valid sample and completed the relevant questionnaires. For the individual questionnaires with incomplete responses, we made phone confirmations and made corrections. There were 664 valid questionnaires, and the response rate was 100.0%. There were no statistically significant differences in oral examination conditions, demographics, socioeconomics, dietary habits, and oral health behaviors between the two groups of children (P > 0.05). After 1.5 years of follow-up, a total of 618 individuals were reached (306 in the I-ReHealth group and 312 in the Duraphat group), with 46 individuals lost to follow-up. The loss-to-follow-up rates in the I-ReHealth group and the Duraphat group were 6.4% (21/327) and 7.4% (25/337) respectively, and the difference in loss-to-follow-up rates was not statistically significant (P > 0.05). The caries rates at baseline for the two groups were 61.8% and 60.6% respectively, with the mean number of decayed teeth being 3.41 ± 4.25 and 3.52 ± 4.36 respectively; there was no statistically significant difference in the caries rates, mean number of decayed teeth, and visible plaque index between the two groups of children (P > 0.05) (Table 2). No enamel hypoplasia was found in all the children. Tab 2 Comparison of baseline oral examination findings between the two groups of children
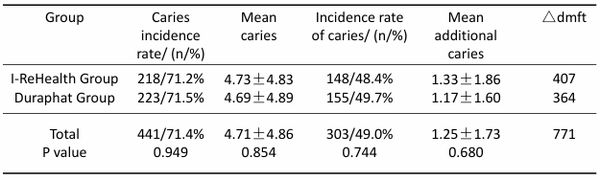
2.2 Pre- and post-intervention caries status After the intervention, there were no statistically significant differences in the caries incidence rate, mean caries number, the incidence rate of caries, and mean additional caries number between the two groups of children (P > 0.05) (Table 3). Tab 3 The caries prevalence, mean dmft, and incidence of new caries in the two groups after 1.5 years
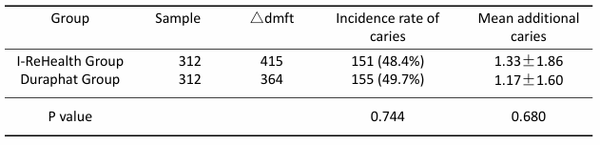
Note: △dmft represents the number of incremental cavities, lost teeth, and filled teeth. 2.3 Non-inferiority test The non-inferiority test results for the mean increase in caries were presented. t=4.940, P < 0.001. The difference in the mean increase in caries between the two groups was 0.16, and the one-sided 97.5% confidence interval of the difference was (-0.114, 0.434). The difference in the mean increase in caries between I-ReHealth and Duraphat was less than the non-inferiority threshold of 0.849, that is, the one-sided 7.5% confidence interval of the difference (-0.114, 0.434) was lower than the non-inferiority threshold. The non-inferiority test was qualified. 2.4 Cost minimization analysis There were no statistically significant differences in the caries incidence rate, mean caries number, the incidence rate of caries between the two groups. However, this does not mean there are no clinical differences. The non-inferiority results prove that the efficacy of I-ReHealth@ is not inferior to Duraphat@, indicating that the caries prevention effect of I-ReHealth@ is at least equivalent to that of Duraphat@. No adverse reactions related to fluoride coatings were found. Therefore, the study uses the cost-minimization analysis method for economic evaluation. Due to the different baseline numbers of the two groups, the total results cannot be directly compared. The standardized baseline numbers need to be standardized, and the standardized results are shown in Table 4. Tab 4 The incidence of new caries in the two groups after 1.5 years of standardization
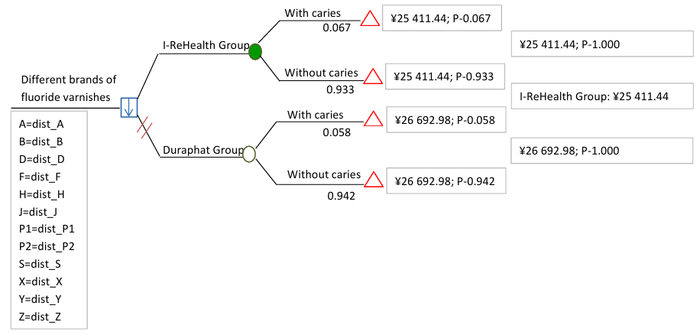
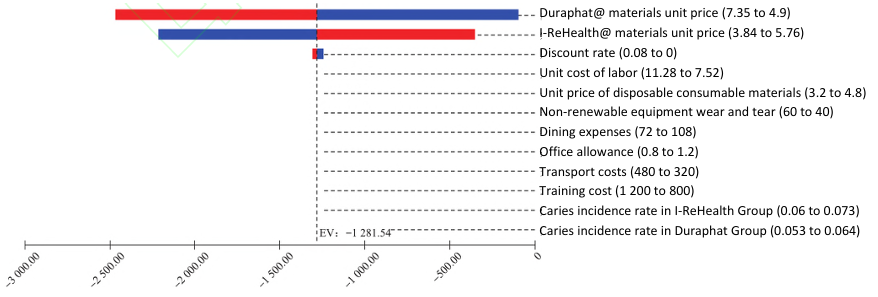
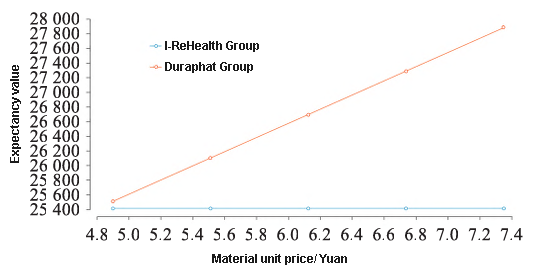
Note: △dmft represents the number of incremental cavities, lost teeth, and filled teeth. After baseline standardization, the total cost of the I-ReHealth group was 25,411.44 yuan, and that of the Duraphat group 26,692.98 yuan. The total cost of the I-ReHealth group was 1,281.54 yuan less than that of the Duraphat group. The specific model after standardization is shown in Figure 2. The cost minimization analysis of the decision tree model indicated that Airecon was the economically preferred option (Figure 3). The single-factor sensitivity analysis shows that the materials of Duraphat@ and I-ReHealth@ have the greatest impact on the results, while the effects of other factors are very small (Figure 4). When these two factors fluctuate within the given range, the total cost of the I-ReHealth group is always lower than that of the Duraphat group, and the outcome is robust (Figures 5 and 6).
Fig 2 Decision tree model for caries prevention with two fluoride varnishes
Fig 3 Cost-minimization analysis of two fluoride varnishes I-ReHealth Group vs. Duraphat Group
Fig 4 Tornado diagram of one-way sensitivity analysis of two fluoride varnishes
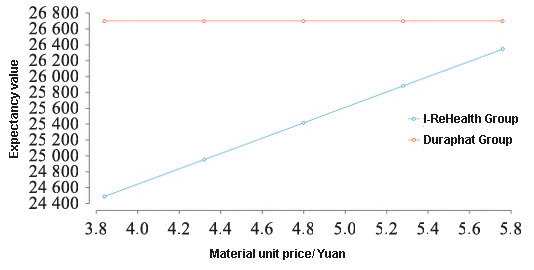
Fig 5 One-way sensitivity analysis of the unit price of I-ReHealth? material
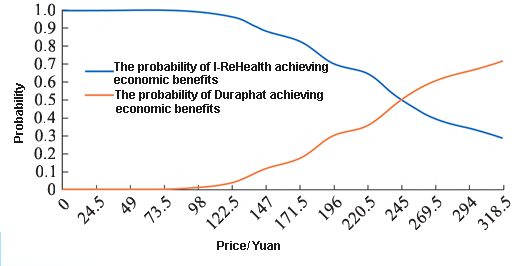
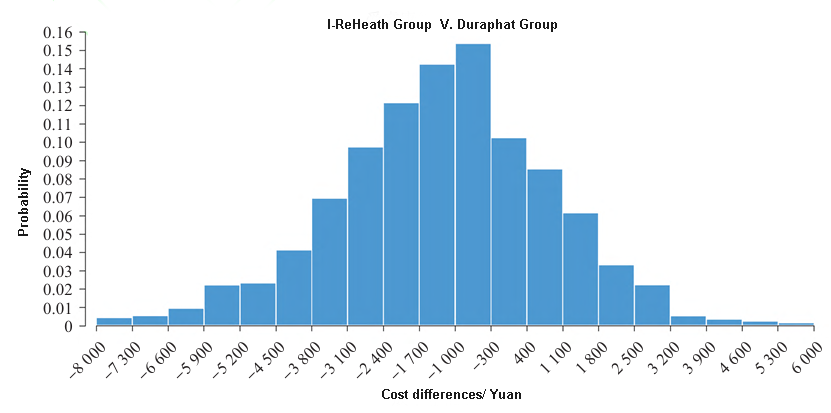
Fig 6 One-way sensitivity analysis of the unit price of Duraphat? material The probability sensitivity analysis shows that as the price of I-ReHealth@ increases, the probability of achieving economic benefits gradually decreases. When the price of i-rehealth@ is lower than 196 yuan, the probability of achieving economic benefits is greater than 70%. When the price of I-ReHealth@ is 245 yuan, the two curves intersect, and the probability of both types of fluoride varnishes being economically viable is 50% (Figure 7). Based on the parameter distribution, 1,000 Monte Carlo simulations were conducted. The results show that the probability of the total cost of the I-ReHealth group being lower than that of the Duraphat group is 73.1%, meaning that in most simulation scenarios, the cost performance of the I-ReHealth@ solution is superior to that of Duraphat@ (Figure 8).
Fig 7 I-ReHealth? compared to Duraphat? price economic probability curve chart
Fig 8 Probability sensitivity analysis of cost differences 3. Discussion The WHO's "Global Action Plan for Oral Health (2023-2030)" emphasizes that optimizing the application of fluoride is one of the key strategies for improving global oral health. At the same time, the "Healthy China 2030" planning outline proposes to promote technological innovation and cost optimization of domestic medical consumables, providing policy support for the research and application of domestic fluoride coatings. I-ReHealth@ fluoride varnish is a domestically produced fluoride protective paint containing 5% sodium fluoride, with a material formula table highly consistent with that of Duraphat@. Its price is cheaper than Duraphat@ and is currently widely used in Guangxi. Since fluoride varnishes fall under the category of Class II medical device products, and are exempt from clinical evaluation in the management directory of the National Medical Products Administration, no relevant evaluation of the anti-caries effect of I-ReHealth@ has been found yet. In order to further assess the anti-caries effect of I-ReHealth@ and conduct a comparative study on the economic benefits of I-ReHealth@ and Duraphat@, this research conducted a systematic evaluation at the kindergarten in Yizhou District, Hechi City, Guangxi Province, using a community intervention trial design. This study, through a community intervention trial, found that there was no statistically significant difference in the incidence of dental caries (48.4% for I-ReHealth@, 49.7% for Duraphat@) and the average number of new caries (1.33 ± 1.86 for I-ReHealth@, 1.17 ± 1.60 for Duraphat@) between the two groups of children. Further non-inferiority testing revealed that the upper limit of the difference in the average number of new caries between I-ReHealth@ and Duraphat@ (0.434) was lower than the non-inferiority threshold (0.849). The research data confirms the validity of the non-inferiority hypothesis, and it can be concluded that I-ReHealth@ and Duraphat@ have comparable effects in preventing dental caries in young children's primary teeth. This result is consistent with the core caries prevention mechanism of fluoride coatings – the enamel remineralization mediated by fluoride ions (22,600 ppm), indicating that the two products have equivalent clinical caries prevention efficacy. Based on this, this study conducted a health economics evaluation using the cost-minimization analysis method, and found that the total intervention cost of the I-Rehealth group (25,411.44 yuan) was lower than that of the Duraphat group (26,692.98 yuan). This finding provides an important basis for choosing more cost-effective caries prevention measures for grassroots public health projects. It should be noted that while conducting medical economic evaluations, there is room for variation in the actual values of economic cost calculation parameters, which leads to uncertainties and deviations in the cost calculation results due to differences in real conditions. The impact of parameter variations on the results can be evaluated through single-factor sensitivity analysis and probabilistic sensitivity analysis. The single-factor sensitivity analysis revealed that the cost of fluoride varnish materials was the main factor contributing to the cost differences between the two groups. The lower material price of I-ReHealth@ enabled it to maintain an advantage in the total cost. Further probability sensitivity analysis (through 1,000 Monte Carlo simulations) indicated that when the material price of I-ReHealth@ was lower than 196 yuan per unit, the probability of its having a cost advantage exceeded 70%. This threshold could provide a quantitative reference for the centralized procurement decisions of the medical insurance department. The overall results of the Monte Carlo simulation show that in 73.1% of the simulation scenarios, the total cost of the I-ReHealth group was lower than that of the Duraphat group. This further validates the robustness of the research conclusion, that is, in most simulated real cost combinations, the total cost of the I-ReHealth group would be lower than that of the Duraphat group. The caries-preventing mechanism of fluoride varnish mainly relies on a dynamic process of "application - penetration - solidification - release". During this process, the fluidity of the material and the solidification time are the key factors affecting its clinical efficacy. Research indicates that if the solidification time is too short, it will reduce the convenience of clinical operation, while if the solidification time is too long, it may affect the adhesion performance of the material to the tooth surface. This study found that although the setting time of I-ReHealth@ was slightly shorter than that of Duraphat@ (possibly due to differences in additive formulation and production process), there was no clinical difference in the anti-caries effect between the two groups. This finding suggests that domestic fluoride- varnish, while ensuring the anti-caries effect, have achieved better clinical operability through process optimization, providing convenience for the anti-caries work in grassroots medical institutions. In terms of safety, although fluoride coatings have a relatively high safety profile in the prevention of dental caries in children, previous studies have reported potential risks such as local irritation and systemic reactions. In this study, by strictly following the product usage guidelines, controlling the single application dose (0.25 g), and implementing standardized operating procedures, no serious adverse reactions were observed during the 1.5-year follow-up period. This result confirms that under standardized community intervention conditions, both types of fluoride varnishes demonstrated excellent safety and tolerance, providing reliable safety evidence for the clinical selection of anti-caries materials. A particularly noteworthy aspect of the results of this study is that although I-ReHealth@ and Duraphat@ have shown certain effects in preventing dental caries, they have failed to effectively curb the rapid increase in the incidence of dental caries among the study population. This phenomenon may be related to various factors such as children's filling of cavities, frequency of sweet food intake, plaque control, and fluoride application frequency. 1) The filling rate of dental caries in children. The research team's previous study based on the caries risk prediction model confirmed that the baseline number of lost and filled teeth was the strongest contributing factor in predicting future caries risk. This highlights the importance of timely filling of decayed primary teeth in the prevention and control of caries. It is worth noting that during the research process, although the oral examination results were reported to the parents and treatment advice notices were issued, most parents still did not bring their children for subsequent treatment. This phenomenon indicates that parents currently have insufficient awareness of the harmfulness of primary tooth caries, and suggests that future efforts are needed to strengthen oral health education for parents. 2) Frequency of consuming sweet foods and plaque control. The baseline survey revealed that nearly 70% of the children consumed sweet foods at least once a day. After regular oral health education conducted every six months, more than half of the children still consumed sweet foods daily. In terms of plaque control, over half of the children had plaque levels exceeding 20%. After intervention, nearly 20% of the children still had poor plaque control, indicating that the frequency of oral health education needs to be increased. 3) Frequency of fluoride application intervention. In this study, we adopted a regular and periodic fluoride application intervention once every six months. If we had selected high-risk individuals and conducted four fluoride applications per year, it would also have affected the intervention outcome. This suggests that fluoride application intervention can to some extent delay and inhibit the development of dental caries. However, relying solely on fluoride application cannot achieve a comprehensive caries prevention effect. Therefore, we should change the prevention and control mindset, explore more scientific, systematic and effective prevention and treatment measures, strengthen oral health education for parents, promote filling of primary teeth caries, strengthen the frequency of oral health education for children, help them establish good oral health habits, and screen high-risk individuals to enhance the frequency of fluoride application intervention. The implementation of multiple measures in a coordinated manner can achieve a more significant caries prevention effect. This study also has certain limitations. 1) The follow-up period is relatively short. Dental caries, as a chronic disease, requires long-term observation. Although the 1.5-year follow-up data in this study showed cost advantages, the research period needs to be extended to verify the long-term effects. 2) Limited sample area. The risk levels of dental caries in the current single-center study samples show a cross-distribution and have regional characteristics. Multi-center large-sample studies are needed to enhance the generalizability of the conclusions. 3) The cost calculation is incomplete. Public costs such as oral health education have not been included in the estimation, which may lead to an underestimation of the actual expenditure. A more comprehensive economic model needs to be established to improve the accuracy. 4) The price data is singular. The analysis based on a single purchasing source (the bidding price of a certain tertiary-level dental specialty hospital) is prone to bias. It is necessary to integrate data from multiple centers to enhance the representativeness of the economic evaluation. In conclusion, I-ReHealth@ cavity prevention effect is not inferior to Duraphat, and it also has significant cost advantages. It is suitable to be the preferred material for large-scale community cavity prevention projects in Hechi City, Guangxi. To further verify the representativeness and applicability of this conclusion, the research team will conduct multi-center studies in multiple locations. Additionally, it is recommended that the health administrative department, when formulating strategies for preventing childhood dental caries, comprehensively consider the cavity prevention effect and economic cost, and prioritize the selection of more cost-effective fluoride coatings to optimize the allocation of public health resources and provide more comprehensive evidence-based basis for policy formulation. Source: West China Journal of Stomatology ISSN 1000-1182,CN 51-1169/R |